Laser Therapy (PDL and Fractional)
Last reviewed: April 2026
Evidence rating reflects the quality and volume of research — not how well the treatment works. How I grade evidence →
Medical-grade lasers — most often pulsed dye laser (585/595 nm) or fractional CO2 and Er:YAG — used by dermatologists to reduce scar redness, soften texture, and open microchannels for laser-assisted drug delivery. Laser is rarely used alone; its strongest evidence is as a potentiator that makes other treatments work better.
How it works
Different laser types work on different scar features. Pulsed dye laser (PDL) at 585-595 nm is absorbed selectively by haemoglobin in the scar's blood vessels, causing photothermolysis of the abnormal vasculature that feeds inflammation and redness; this reduces TGF-β signalling and visible erythema. Fractional ablative lasers (CO2 at 10,600 nm, Er:YAG at 2940 nm) vaporize tiny columns of tissue, leaving untreated skin between them to speed healing — the microscopic wounds trigger collagen remodelling and, crucially, create open channels that let topically applied triamcinolone or 5-FU penetrate into the scar. This technique, called laser-assisted drug delivery (LADD), is the main reason fractional lasers have become a standard tool in keloid clinics. Non-ablative fractional lasers (e.g. 1550 nm, 1927 nm) use the same channel-based concept but without vaporizing tissue, trading slower results for less downtime and lower pigmentation risk.
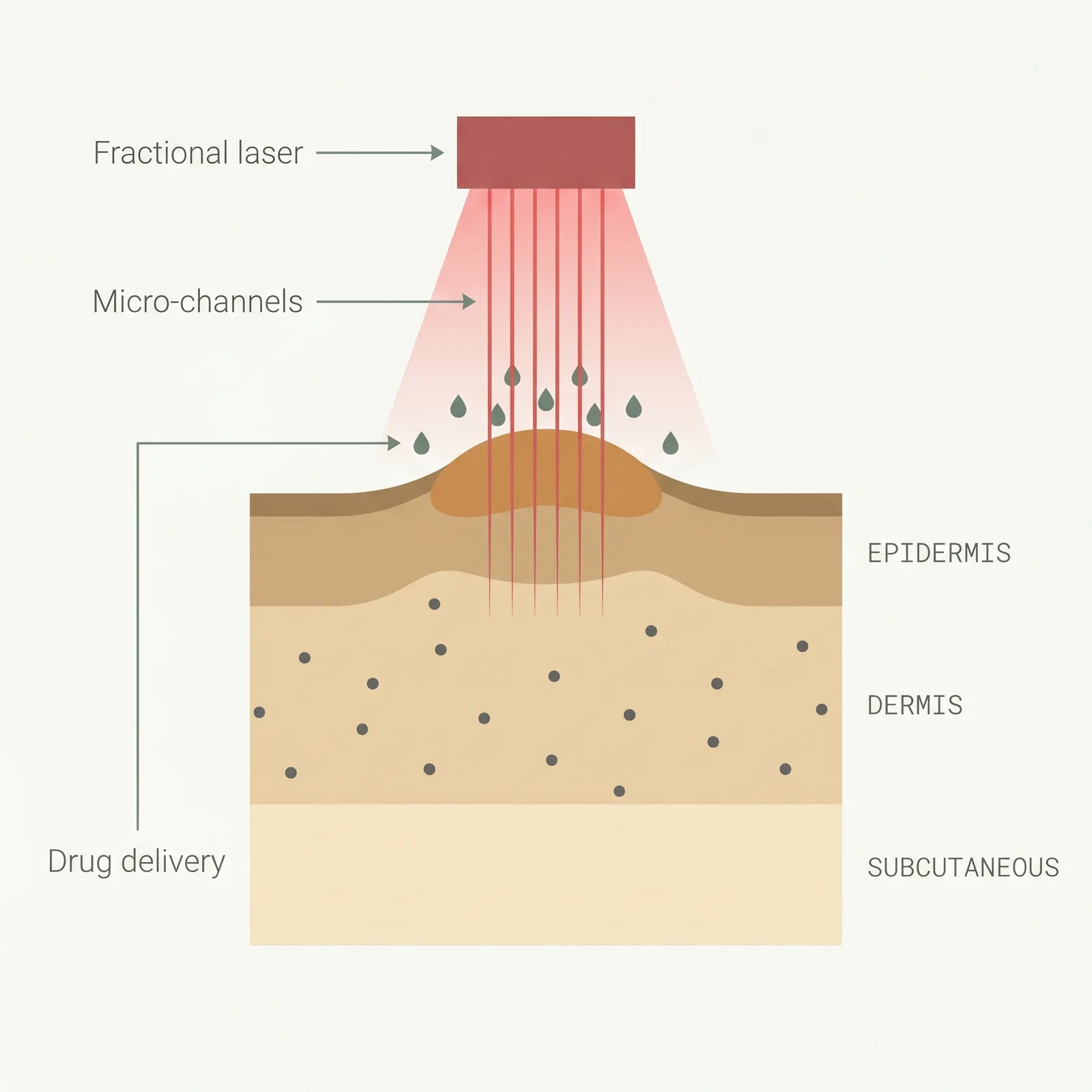
- 1Targeted light. Pulsed dye (PDL) targets blood vessels in red, inflamed scars; fractional lasers remodel collagen.
- 2Micro-channels. Fractional ablative lasers cut tiny columns through the scar, stimulating remodeling with minimal downtime.
- 3Drug delivery. The open channels let topical steroid or 5-FU reach deeper scar tissue — better outcomes than laser alone.
Typical protocol
PDL: 4-6 sessions at 4-6 week intervals for redness-driven hypertrophic scars. Fractional ablative: 3-5 sessions at 6-8 week intervals, often immediately followed by topical or intralesional steroid/5-FU (LADD). Dermatologists commonly layer PDL and fractional lasers in alternating visits for scars that are both red and thick.
- Time to results
- Redness reduction visible in weeks; textural improvement over 3-9 months of consistent sessions.
- Accessibility
- specialist required
- Recurrence
- Variable — laser is usually used to augment another primary therapy rather than define long-term recurrence on its own
- Insurance
- rarely
Best for
- • Red, inflamed hypertrophic scars where PDL can target scar vasculature
- • Thick, mature keloids where laser-assisted drug delivery (LADD) is planned alongside steroid or 5-FU
- • Facial, neck, and chest scars where cosmetic outcome matters
- • Scars that have plateaued on injections or silicone alone
- • Post-surgical scars entering the remodelling phase (3-12 months post-op)
- • Burn scars with both pigmentary and textural concerns
Limitations to know
Combining with other treatments
Laser-assisted drug delivery (LADD) is the protocol with the strongest supporting evidence: a fractional ablative pass is followed immediately by topical or intralesional triamcinolone and/or 5-FU applied over the treated area. The open microchannels let the drug reach far deeper and more evenly than a standard injection, which is especially useful for thick plaque-like keloids that are hard to inject. PDL is often layered on top of steroid/5-FU protocols to quiet redness and itch between injection visits. Red-light therapy at home between sessions is commonly used to support recovery and extend the anti-inflammatory effect. Laser is not typically paired with radiation therapy in the same course.
Evidence sources
Laser Treatment of Hypertrophic Scars, Keloids, and Striae
2003Nouri K, Jimenez GP, Harrison-Balestra C, Elgart GW · Dermatologic Surgery
Pulsed dye laser produced meaningful improvement in scar erythema, pliability, and patient-reported outcome, establishing PDL as a foundational tool for red/inflamed scars.
View source →Laser-Assisted Drug Delivery for Hypertrophic Scars and Keloids
2019Waibel JS, Rudnick A, Shagalov DL, Nicolazzo DM · Dermatologic Surgery
Fractional ablative laser followed by topical corticosteroid (LADD) improved scar height, texture, and pliability metrics compared with laser or steroid alone.
View source →Laser Treatment of Traumatic Scars With an Emphasis on Ablative Fractional Laser Resurfacing: Consensus Report
2014Anderson RR, Donelan MB, Hivnor C, et al. · JAMA Dermatology
Multi-specialty consensus recommending ablative fractional lasers as a primary tool for traumatic and surgical scar remodeling, particularly in combination with intralesional medication.
View source →Pulsed Dye Laser Versus Intralesional Triamcinolone for Hypertrophic Scars: A Randomized Comparison
1995Alster TS, Williams CM · Lancet
PDL produced significant improvement in scar erythema, pliability, and pruritus with fewer side effects than intralesional steroid alone — one of the earliest randomized trials supporting laser for scar management.
View source →
Frequently asked questions
Is laser therapy safe for darker skin tones?
It depends on the laser. Pulsed dye laser can be used across skin tones with careful settings but still carries a real risk of post-inflammatory hyperpigmentation in Fitzpatrick IV-VI. Ablative fractional CO2 at aggressive settings is higher risk in darker skin; many practitioners prefer non-ablative fractional lasers (1550 nm or 1927 nm), longer cooling, and lower fluences. Always ask for a test spot in an inconspicuous area and wait 4-8 weeks before committing to a full treatment. If the clinic won't do a test spot or can't show experience with skin types IV-VI, find a different provider.
What is laser-assisted drug delivery (LADD) and why is it a big deal?
LADD uses a fractional ablative laser to punch microscopic channels into the scar, then applies topical or intralesional triamcinolone or 5-FU immediately over the same area. The open channels let the medication reach far deeper and more evenly than a standard needle injection, which matters most for thick, plaque-like keloids where needle injections struggle to distribute the drug. Published trials consistently show LADD outperforms either laser or injection alone, and it's become the standard approach for resistant or large keloids in many dermatology clinics.
How is laser therapy different from red light therapy?
Different tool, different purpose. Medical lasers are high-intensity, precisely targeted devices that cause controlled tissue damage (PDL targets vessels, fractional lasers vaporize tissue) to trigger remodelling. Red light therapy (photobiomodulation) is low-intensity LED light that feeds cellular energy production without tissue damage. Laser is a clinical procedure with downtime and recurrence risk; red light is a daily at-home adjunct with no downtime. They're often used together — laser in the clinic every few weeks, red light at home every day to support recovery and extend the anti-inflammatory effect.
How many laser sessions will I need?
Most protocols run 4-6 sessions for PDL at 4-6 week intervals, or 3-5 sessions for fractional ablative at 6-8 week intervals. Response is usually assessed at the halfway point; if the scar is clearly improving, the schedule continues. Thick or long-standing keloids often need more sessions and combination with LADD or injections. If cost is a barrier, pairing a smaller number of laser sessions with consistent at-home silicone and red-light therapy is more cost-effective than pushing for more laser visits alone.
What is the downtime after fractional laser?
Ablative fractional (CO2, Er:YAG): 3-10 days of redness, swelling, pinpoint bleeding, and crusting, with pink skin lasting 2-4 weeks. Avoid sun exposure strictly during this window and wear high-SPF sunscreen for at least 3 months post-session to prevent hyperpigmentation. Non-ablative fractional and PDL: usually 1-3 days of redness and mild swelling with no crusting. Bruising from PDL (purpura) can last up to a week at higher fluences. Plan sessions with at least a week of low social exposure if you can.
Medical disclaimer
ScarInsight provides educational information about scar and keloid treatments based on published research. This content is not intended to diagnose, treat, or prevent any medical condition. Individual results vary. Treatment decisions should be made in consultation with a qualified dermatologist or healthcare provider who can evaluate your specific situation. ScarInsight is not a healthcare provider and does not offer medical advice.