Intralesional Steroid Injections (Triamcinolone)
Last reviewed: April 2026
Evidence rating reflects the quality and volume of research — not how well the treatment works. How I grade evidence →
Direct injection of corticosteroid (usually triamcinolone acetonide) into keloid tissue to flatten and soften the scar. Considered first-line for many keloid presentations.
How it works
Triamcinolone is a potent long-acting corticosteroid that does three things simultaneously when deposited inside a keloid. First, it suppresses the hyperactive fibroblasts that drive collagen overproduction, the core mechanism of keloid growth. Second, it down-regulates TGF-β1 signalling and up-regulates collagenase, which means less new scar tissue is laid down and some of the existing excess collagen is actively broken down. Third, it calms the local inflammatory environment — reducing the itching, tenderness, and burning sensation that many keloid patients find just as disabling as the visible scar. The effect is cumulative across multiple sessions, which is why protocols run 3-6 injections rather than one. It does not remove the scar — it shrinks and softens it — and combining with cryotherapy (to soften dense tissue first) or 5-FU (to add anti-proliferative action) generally outperforms triamcinolone alone.
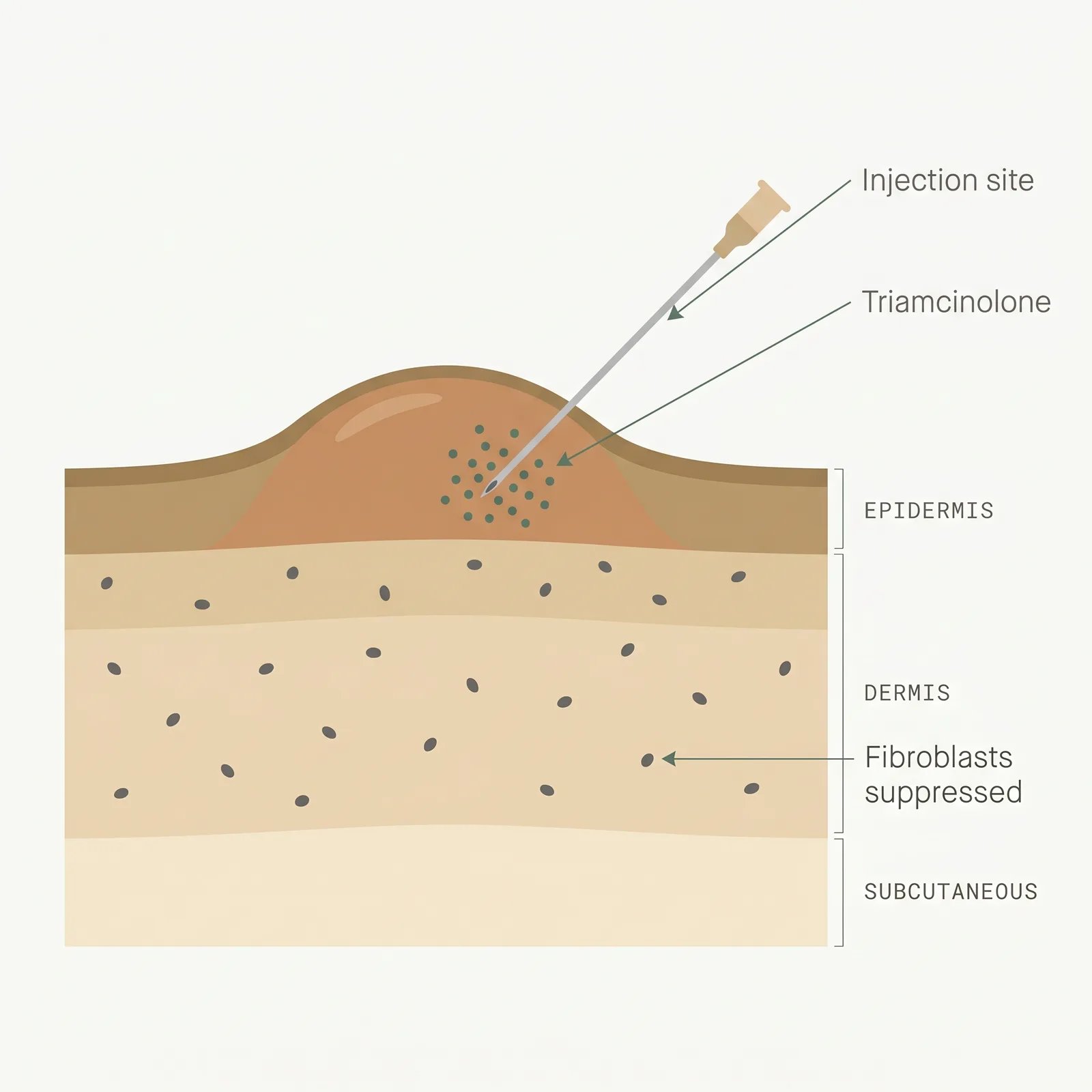
- 1Direct delivery. A fine needle places triamcinolone inside the dense scar core where oral or topical drugs can’t reach.
- 2Fibroblast suppression. The steroid inhibits fibroblast proliferation and collagen synthesis while calming local inflammation.
- 3Gradual flattening. Repeated sessions every 4–8 weeks reduce scar height, itch, and tenderness over 3–6 months.
Typical protocol
Every 4-8 weeks for 3-6 sessions. Concentrations commonly range from 10 to 40 mg/mL, adjusted by scar thickness and location.
- Time to results
- Softening often within 4-6 weeks; visible flattening over 3-6 months.
- Accessibility
- widely available
- Recurrence
- 20-50% when used alone; lower when combined with surgery or 5-FU
- Insurance
- often
Best for
- • Small to medium keloids
- • Ear keloids (lobe and cartilage)
- • Symptomatic keloids (itching, tenderness)
- • First-line treatment before considering surgery
Limitations to know
Combining with other treatments
Triamcinolone is the workhorse of keloid care and pairs well with almost every other modality. Post-excision steroid protocols (starting 2-4 weeks after surgery, continuing every 4-6 weeks for 6-12 months) are one of the most reliable ways to reduce surgical recurrence. Cryo-assisted steroid injection uses a brief contact freeze just before the needle goes in, which softens dense tissue and lets the drug disperse more evenly — this often allows a lower steroid dose with less atrophy risk. Combination with 5-fluorouracil (the 9:1 5-FU/triamcinolone mix) outperforms plain steroid on flattening and itch in randomized trials, and reduces steroid-related side effects because less steroid is needed overall. Silicone sheeting and red-light therapy are commonly layered on as daily background care between injection visits.
Evidence sources
Updated International Clinical Recommendations on Scar Management
2014Gold MH, Berman B, Clementoni MT, et al. · Dermatologic Surgery
International consensus lists intralesional corticosteroid as a first-line option for keloid management.
View source →Keloid and Hypertrophic Scars: A Review
2022Ogawa R · Plastic and Reconstructive Surgery
Triamcinolone remains a foundational therapy; combination protocols yield better long-term control than monotherapy.
View source →Intralesional Triamcinolone Alone or in Combination for Keloid Treatment
2019Khalid FA, Mehrose MY, Saleem M, et al. · Burns
Combination with 5-fluorouracil outperformed triamcinolone alone on scar height, pliability, and pruritus.
View source →Efficacy of Intralesional Triamcinolone Acetonide in the Treatment of Keloids: A Systematic Review
2018Morelli Coppola M, Salzillo R, Segreto F, Persichetti P · Clinical, Cosmetic and Investigational Dermatology
Systematic review covering 3,000+ treated keloids found triamcinolone produced improvement in roughly 50-100% of cases depending on protocol and site, with combination therapy consistently outperforming monotherapy.
View source →Local Side Effects of Intralesional Corticosteroid Injections
2014Lee EJ, Jung SY, Lee SJ, et al. · Dermatologic Surgery
Skin atrophy, hypopigmentation, and telangiectasia are dose- and frequency-dependent; lower concentrations (10 mg/mL) and longer intervals between injections reduce side effect rates substantially without sacrificing efficacy.
View source →
Frequently asked questions
How painful are steroid injections?
Most patients describe the injection as a sharp pinch followed by pressure, typically rated 3 to 4 out of 5. Dense keloid tissue resists injection, which can make it sting more than a typical shot. Dermatologists often apply topical anesthetic or use ice first, and some use a pressure device to reduce discomfort.
How many sessions will I need?
Most protocols run 3 to 6 sessions spaced 4 to 8 weeks apart. Small or responsive keloids may settle in 3 sessions, while dense or recurrent keloids can need more. If a keloid has not responded after 3 sessions, that is usually a signal to step up to a combination protocol rather than continue monotherapy.
What are the most common side effects?
Local side effects include skin thinning (atrophy), hypopigmentation (lighter skin), and small visible blood vessels (telangiectasia) at the injection site. These are more common with higher concentrations or frequent injections. Systemic effects are rare at standard keloid doses, but raise any changes in menstrual cycle, weight, or mood with your dermatologist.
Will steroid injections alone remove my keloid?
Unlikely for mature or large keloids. Steroids flatten and soften scar tissue and reduce symptoms, but they rarely erase an established keloid. The better mental model is that injections shrink and calm the scar. Combination with silicone, surgical excision, or 5-fluorouracil gives the best long-term results.
Are steroid injections covered by insurance?
Often yes when the keloid is symptomatic (itching, pain, obstruction) and the procedure is billed as medically necessary. Cosmetic-only cases are less likely to be covered. Ask the office to verify benefits before the first session and ask for the CPT code they plan to submit so you can check with your insurer.
Medical disclaimer
ScarInsight provides educational information about scar and keloid treatments based on published research. This content is not intended to diagnose, treat, or prevent any medical condition. Individual results vary. Treatment decisions should be made in consultation with a qualified dermatologist or healthcare provider who can evaluate your specific situation. ScarInsight is not a healthcare provider and does not offer medical advice.