5-Fluorouracil (Intralesional)
Last reviewed: April 2026
Evidence rating reflects the quality and volume of research — not how well the treatment works. How I grade evidence →
An antimetabolite chemotherapy agent used at very low doses and injected directly into keloid tissue, most often paired with a small amount of triamcinolone. 5-FU is the usual next step when steroid injections alone have stalled, and the combination produces better flattening with fewer steroid-related side effects than triamcinolone monotherapy.
How it works
5-FU blocks thymidylate synthase, the enzyme fibroblasts need to synthesize DNA. In keloid tissue this selectively suppresses the hyperactive fibroblasts driving scar expansion, reduces TGF-β signaling, and down-regulates type I collagen production — the three mechanisms most linked to keloid growth. At the low concentrations used for intralesional scar work (typically 50 mg/mL, delivered in microlitre doses), 5-FU reaches a therapeutic local effect without meaningful systemic exposure: blood levels after a keloid session are a fraction of oncology dosing. Combining with a small amount of triamcinolone (the common 9:1 ratio) adds an anti-inflammatory signal on top of the anti-proliferative one, and also lets the dermatologist use a much lower steroid dose — which is why combination therapy produces less skin atrophy, hypopigmentation, and telangiectasia than pure steroid regimens.
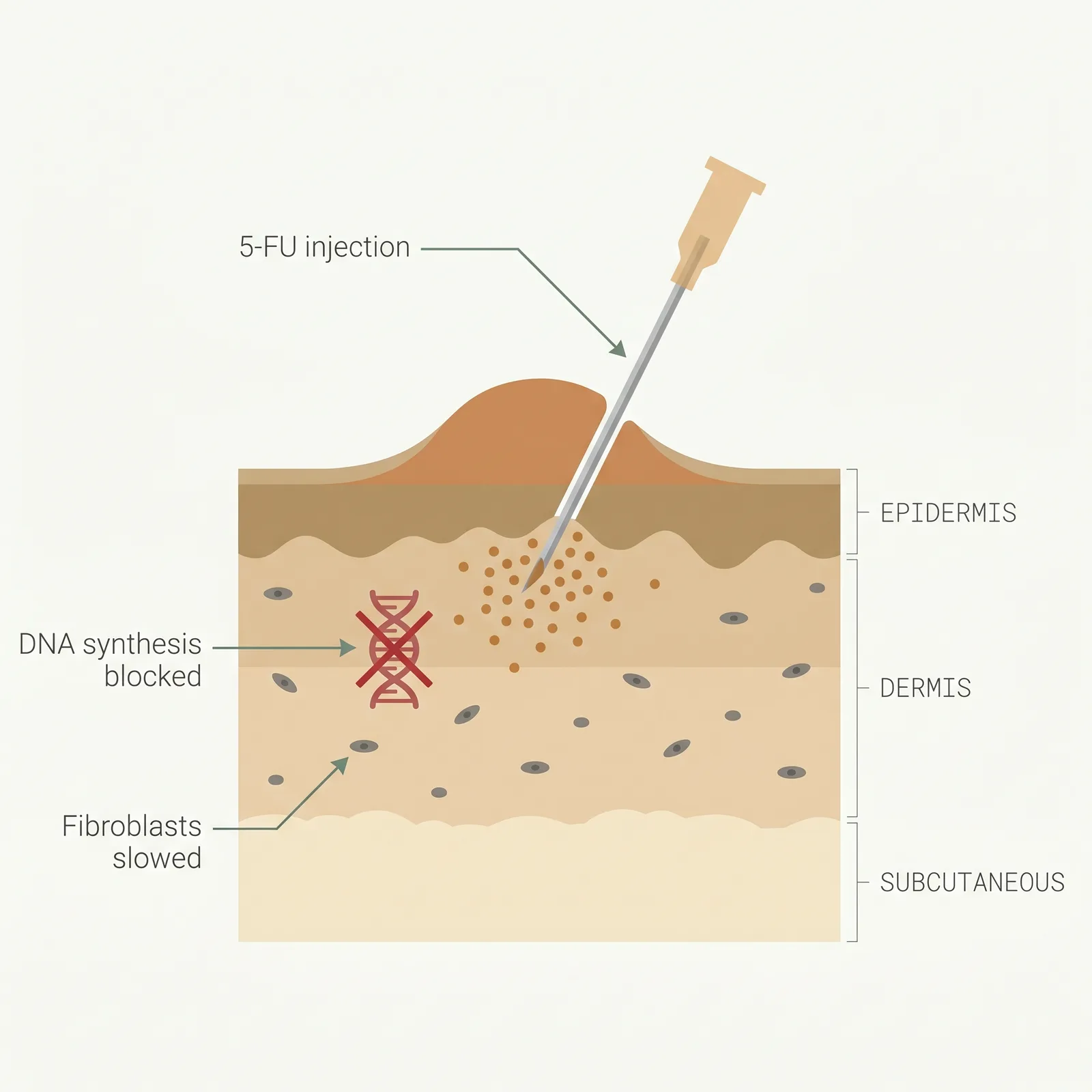
- 1Antimetabolite, placed inside. Low-dose 5-FU is injected directly into the keloid, often alongside a small amount of triamcinolone.
- 2Blocks DNA synthesis. 5-FU interferes with the DNA replication that fibroblasts need to proliferate and lay down collagen.
- 3Steroid-sparing. Useful when keloids resist steroid alone, or when steroid atrophy is a concern — combo outperforms either.
Typical protocol
Weekly or biweekly injections for 6-12 sessions, most commonly in a 9:1 ratio of 5-FU (50 mg/mL) to triamcinolone (40 mg/mL). Some protocols move to every 4 weeks once the scar softens. Total 5-FU per session is usually capped at around 50-100 mg to stay well within systemic safety margins.
- Time to results
- Softening and reduction in itch often in the first 4-6 weeks; visible flattening over 2-4 months of consistent dosing.
- Accessibility
- specialist required
- Recurrence
- 20-40% as monotherapy; 10-20% in combination with triamcinolone or post-excision
- Insurance
- sometimes
Best for
- • Steroid-resistant keloids that have not responded after 3-4 triamcinolone sessions
- • Patients where steroid-induced atrophy, telangiectasia, or hypopigmentation is a concern
- • Adjunct to surgical excision (post-op injection protocols)
- • Keloids that continue to itch, grow, or flare despite steroid injections
- • Young, actively growing keloids in the first 12 months
- • Patients with darker skin tones where steroid pigmentation change is more visible
Limitations to know
Combining with other treatments
The best evidence for 5-FU is in combination, not alone. The 9:1 5-FU/triamcinolone mix has become the default in many keloid clinics because it outperforms either agent alone and reduces steroid side effects at the same time. 5-FU also pairs well with surgical excision — post-op injection protocols (starting within 2-4 weeks of surgery and continuing for 6-12 months) are a common strategy for high-risk, recurrent keloids that aren't suitable for radiation. Some clinics add pulsed dye laser in the same session to target scar vasculature and inflammation alongside the fibroblast suppression from 5-FU. Silicone sheeting and red-light therapy are commonly layered on as daily background care between injection visits.
Evidence sources
Intralesional 5-Fluorouracil for Keloids and Hypertrophic Scars: A Review
2016Shah VV, Aldahan AS, Mlacker S, et al. · Dermatologic Surgery
Review of multiple trials found 5-FU alone or combined with steroid reduced scar volume and symptoms with an acceptable side-effect profile; combination protocols outperformed monotherapy across most endpoints.
View source →Intralesional Triamcinolone Acetonide Versus Combination With 5-Fluorouracil
2014Khan MA, Bashir MM, Khan FA · Journal of the Pakistan Medical Association
Combination therapy produced greater scar flattening and fewer steroid-related side effects (atrophy, telangiectasia, hypopigmentation) than triamcinolone alone.
View source →Intralesional Triamcinolone Alone or in Combination With 5-Fluorouracil for Keloid Treatment
2019Khalid FA, Mehrose MY, Saleem M, et al. · Burns
Randomized comparison showed combination 5-FU plus triamcinolone outperformed triamcinolone alone on scar height, pliability, and pruritus scores at 6 months.
View source →Combination of 5-Fluorouracil, Triamcinolone, and Pulsed Dye Laser for Keloid Scars
2006Asilian A, Darougheh A, Shariati F · Dermatologic Surgery
Triple therapy (5-FU + triamcinolone + pulsed dye laser) produced higher rates of >50% improvement than 5-FU + triamcinolone alone, and meaningfully outperformed triamcinolone monotherapy.
View source →
Frequently asked questions
Is 5-FU safe for a scar? It sounds like chemotherapy.
It is a chemotherapy drug, but the dose used for keloids is a tiny fraction of oncology dosing. A typical keloid session uses 50-100 mg delivered locally into the scar; systemic chemo regimens use 500-1000 mg or more delivered into the bloodstream over a cycle. Blood levels after an intralesional injection are very low, and published trials show no bone marrow or immune suppression at keloid doses. The main risks are local: injection pain, ulceration, and temporary hyperpigmentation. It should still be avoided in pregnancy and in people with active infection or bone marrow suppression.
When should I switch from plain steroid injections to 5-FU?
The usual trigger is 3-4 triamcinolone sessions without a meaningful response, or earlier if the keloid is actively growing, very dense, or already developing steroid side effects like skin thinning, telangiectasia, or hypopigmentation. Combination 5-FU plus a lower dose of triamcinolone is often the next step because it adds anti-proliferative action while reducing the total steroid burden. If you are on your third or fourth steroid session and the scar isn't budging, it's reasonable to ask your dermatologist about switching protocols.
How painful are 5-FU injections compared to steroid injections?
Roughly similar — a 3-4 out of 5 — but 5-FU tends to cause more of a burning or aching sensation during and after injection, whereas straight steroid feels more like pressure. Some patients report throbbing or soreness at the site for 24-48 hours. Topical anaesthetic applied 30-60 minutes before the appointment, cold compresses, and slow injection technique all help. Most people find the side effect profile more tolerable than straight steroid because there is less skin thinning.
How many sessions will I need with 5-FU?
Most protocols run 6-12 sessions, initially weekly or biweekly, then spaced to every 3-4 weeks once the scar begins to respond. Response is usually assessed at the 4-6 session mark — if the keloid has flattened and softened, the schedule typically stretches out; if it hasn't moved, your dermatologist may escalate to a different protocol rather than continue indefinitely. Maintenance injections every 2-3 months are sometimes used after initial success to prevent rebound.
Can I get pregnant while on 5-FU injections?
No. 5-FU is teratogenic and is contraindicated during pregnancy and breastfeeding, even at the low intralesional doses. Most clinicians pause treatment if you are trying to conceive and recommend effective contraception throughout the course plus a washout period afterward. Talk to the prescribing clinician about timing if family planning is on your horizon. Plain steroid injections or silicone-based regimens are the usual alternatives during pregnancy.
Medical disclaimer
ScarInsight provides educational information about scar and keloid treatments based on published research. This content is not intended to diagnose, treat, or prevent any medical condition. Individual results vary. Treatment decisions should be made in consultation with a qualified dermatologist or healthcare provider who can evaluate your specific situation. ScarInsight is not a healthcare provider and does not offer medical advice.