Surgical Excision
Last reviewed: April 2026
Evidence rating reflects the quality and volume of research — not how well the treatment works. How I grade evidence →
Physical removal of keloid tissue by a dermatologic or plastic surgeon. Produces immediate volume reduction — but excision alone has one of the highest recurrence rates in all of dermatology (45-100%) because the trauma of surgery itself often triggers a larger keloid. Surgery is only a good idea when it is paired with an aggressive post-op adjunct protocol: steroid injections, radiation, pressure therapy, or a combination.
How it works
The surgeon removes the keloid using one of two approaches. Intralesional excision leaves a thin rim of keloid tissue behind and closes within the scar margin — this reduces wound tension and is favoured for high-risk anatomy. Extralesional excision removes the keloid plus a small margin of normal tissue to make the closure cleaner, at the cost of creating a wound in previously healthy skin. Both techniques aim to close with minimal tension, because tension is one of the strongest mechanical drivers of keloid formation. Without a post-op adjunct, the raw wound triggers exactly the fibroblast cascade that built the original keloid — often producing a larger, more aggressive recurrence along the entire surgical scar line. The adjunct (radiation, steroid, 5-FU, pressure, or more than one) is what interrupts that cascade, which is why surgeons who treat keloids do not offer excision without a defined adjunct plan built into the consultation.
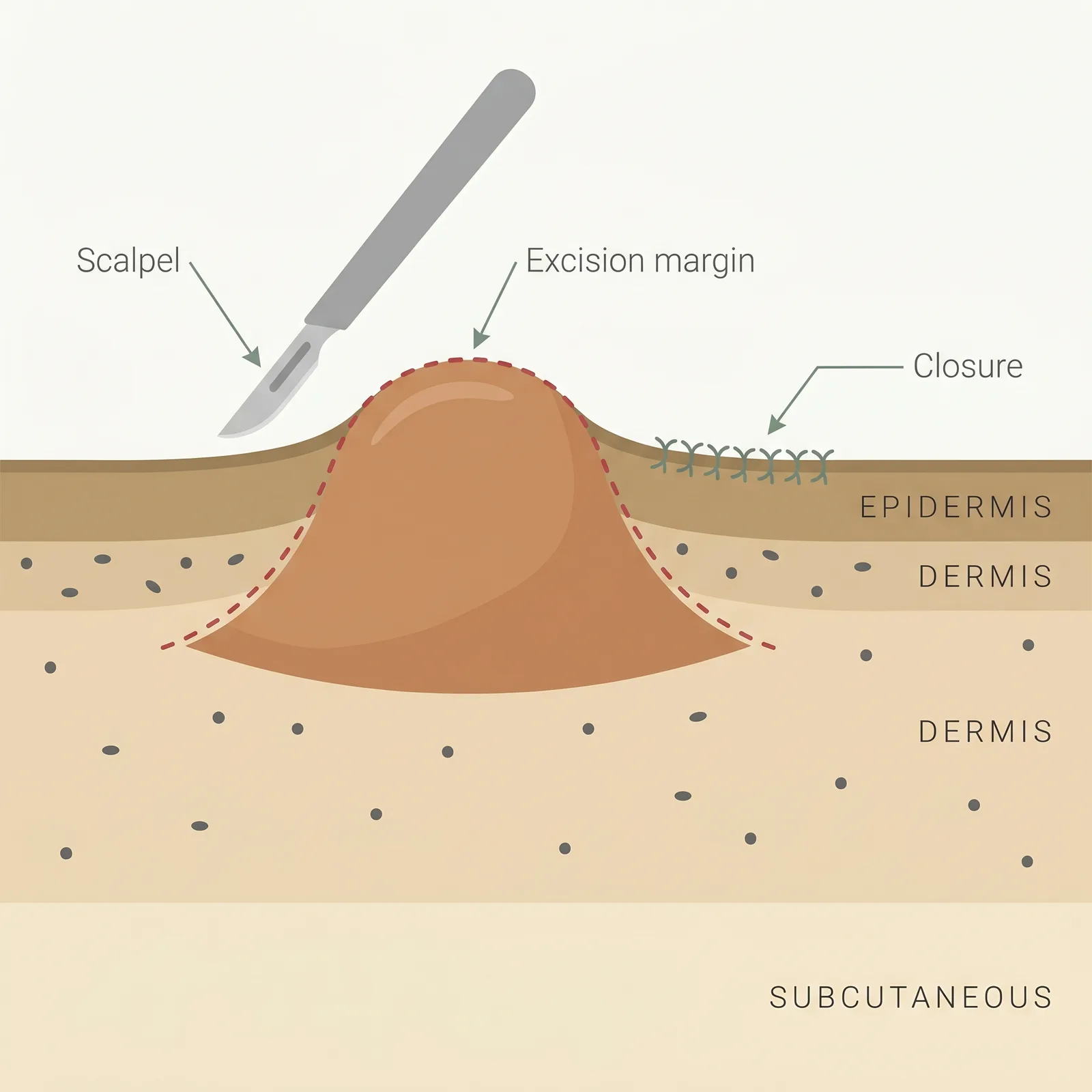
- 1Planned excision. The keloid is removed either within its margin (intralesional) or just beyond it, depending on site and size.
- 2Tension-minimized closure. The wound is closed carefully — high tension itself can trigger a fresh keloid at the scar line.
- 3Adjunct therapy is essential. Excision alone has very high recurrence. Post-op steroid, radiation, or pressure is added within days.
Typical protocol
Single outpatient procedure under local anaesthesia. Post-op adjunct protocols run 6-12 months and most commonly include: intralesional triamcinolone injections starting at 2-4 weeks post-op and continuing every 4-6 weeks; post-op radiation starting within 24-72 hours (for high-risk keloids); or long-term pressure therapy (for ear and extremity sites).
- Time to results
- Immediate volume reduction; long-term outcome judged at 12-24 months based on recurrence.
- Accessibility
- specialist required
- Recurrence
- 45-100% with surgery alone; 10-30% with a proper adjunct protocol (steroid, radiation, pressure, or combination)
- Insurance
- sometimes
Best for
- • Large, bulky, or pedunculated (stalk-like) keloids unlikely to respond to injections alone — especially earlobe keloids
- • Keloids causing functional impairment, obstruction, or chronic ulceration
- • Keloids that have already failed injection and laser protocols
- • Mature keloids that have been stable for at least 12 months (active, growing keloids are higher-risk for aggressive recurrence)
- • Patients committed to the full multi-month post-op adjunct schedule
- • Cases where volume reduction is essential to restoring normal anatomy (e.g. ear reconstruction)
Limitations to know
Combining with other treatments
The evidence overwhelmingly supports combining excision with at least one adjunct. The most common combinations: (1) excision + post-op intralesional triamcinolone every 4-6 weeks for 6-12 months — the default for earlobe, scalp, and smaller keloids; (2) excision + post-op radiation (electron beam or brachytherapy starting within 24-72 hours) — used for recurrent, large, or high-tension-site keloids where radiation centres are accessible; (3) excision + long-term pressure therapy — essential for ear keloids, often layered with steroid injections; (4) excision + post-op 5-FU + triamcinolone — an option for patients who want to avoid radiation but need more than steroid alone. Silicone sheeting begins once the wound is fully closed (usually 2-3 weeks post-op) and continues for 6 months as a low-friction daily layer.
Evidence sources
Keloids: A Review of Etiology, Prevention, and Treatment
2017Berman B, Maderal A, Raphael B · Dermatologic Surgery
Surgical excision combined with adjunctive therapy is consistently more effective than excision alone; recurrence without any adjunct is reported as high as 100% at 12 months depending on site and technique.
View source →The Most Current Algorithms for the Treatment and Prevention of Hypertrophic Scars and Keloids
2010Ogawa R · Plastic and Reconstructive Surgery
Site-specific treatment algorithms combine excision with radiation, steroid, or pressure therapy depending on anatomy, tension, and recurrence risk — now the mainstream approach to surgical planning in keloid care.
View source →Earlobe Keloid Excision Combined With Pressure Therapy
2013Park TH, Rah DK · Archives of Plastic Surgery
Excision plus sustained postoperative compression reduced ear keloid recurrence to the 10-20% range, compared with 45-80% for excision alone.
View source →Updated Scar Management Practical Guidelines
2014Monstrey S, Middelkoop E, Vranckx JJ, et al. · Journal of Plastic, Reconstructive & Aesthetic Surgery
International guidelines explicitly recommend against isolated surgical excision of keloids outside of specific anatomical exceptions; adjunct therapy should be planned before surgery, not after.
View source →
Frequently asked questions
If I just cut this keloid off, will it come back?
Almost certainly, yes — and often bigger. Surgical excision alone has recurrence rates of 45-100% depending on the site, size, and how the wound heals. The trauma of cutting into scar-prone tissue often triggers a larger, more aggressive keloid along the entire surgical scar. This is why reputable dermatologists and plastic surgeons won't offer excision without a defined post-op adjunct plan. If a surgeon offers to just remove a keloid with no follow-up therapy, treat it as a red flag and get a second opinion.
What post-op treatment will I need, and for how long?
At minimum, expect a 6-12 month adjunct protocol. The most common options: intralesional triamcinolone injections every 4-6 weeks (starting around week 2-4 post-op), post-op radiation delivered within 24-72 hours of surgery (for high-risk cases), or continuous pressure therapy for ear keloids. Many protocols combine two or more of these. Silicone sheeting typically starts once the wound closes (2-3 weeks) and continues for 6 months. Skipping the adjunct is the single biggest predictor of recurrence — the 10-30% recurrence rate only holds if you complete the full protocol.
Which sites are hardest to treat surgically?
High-tension areas carry the highest recurrence risk even with full adjunct therapy: the chest (especially sternum), shoulders, upper back, deltoid region, and suprapubic area. These sites have intrinsic skin tension that mechanically drives the keloid cascade, and surgery alone on these sites routinely produces a worse keloid than the original. Earlobes are at the opposite end — low-tension, amenable to clean closure, and respond very well to excision plus steroid or pressure therapy. For a high-tension keloid, many specialists will recommend non-surgical approaches first and only consider excision if it is combined with post-op radiation.
How do I find a surgeon who actually specializes in keloids?
Look for a dermatologic surgeon, plastic surgeon, or facial plastic surgeon who specifically lists keloid or scar revision as a focus area. Ask three practical questions during consultation: roughly how many keloid excisions do they do per year, what is their standard post-op adjunct protocol, and do they work with a radiation oncologist for high-risk cases. A confident, specific answer to each is what you want. 'We'll figure it out after surgery' is not. Academic medical centres and specialty keloid clinics are often better equipped than general practices, particularly for recurrent or high-tension cases.
What's the recovery like?
For a small earlobe excision, recovery is a week or two of mild tenderness with sutures removed around day 7-10. Larger excisions on the chest, shoulder, or back can involve 2-4 weeks of discomfort, activity restrictions to limit wound tension, and 6-8 weeks before you can resume full exercise. If you have post-op radiation, it starts within 24-72 hours and adds 3-5 outpatient sessions in the first week. Expect the wound to remain pink and slightly thickened for several months before maturing — some of this is normal post-surgical change, not recurrence. Your surgeon will tell you what to watch for during the critical 6-12 month window when recurrence, if it happens, usually appears.
Medical disclaimer
ScarInsight provides educational information about scar and keloid treatments based on published research. This content is not intended to diagnose, treat, or prevent any medical condition. Individual results vary. Treatment decisions should be made in consultation with a qualified dermatologist or healthcare provider who can evaluate your specific situation. ScarInsight is not a healthcare provider and does not offer medical advice.