Post-Excision Radiation Therapy
Last reviewed: April 2026
Evidence rating reflects the quality and volume of research — not how well the treatment works. How I grade evidence →
Low-dose radiation — most often superficial electron beam or high-dose-rate brachytherapy — delivered to the fresh surgical site within 24-72 hours after a keloid is excised. It is the most effective recurrence-reduction protocol in the literature for high-risk, recurrent, or large keloids, and is reserved for cases that have failed or would likely fail less aggressive approaches.
How it works
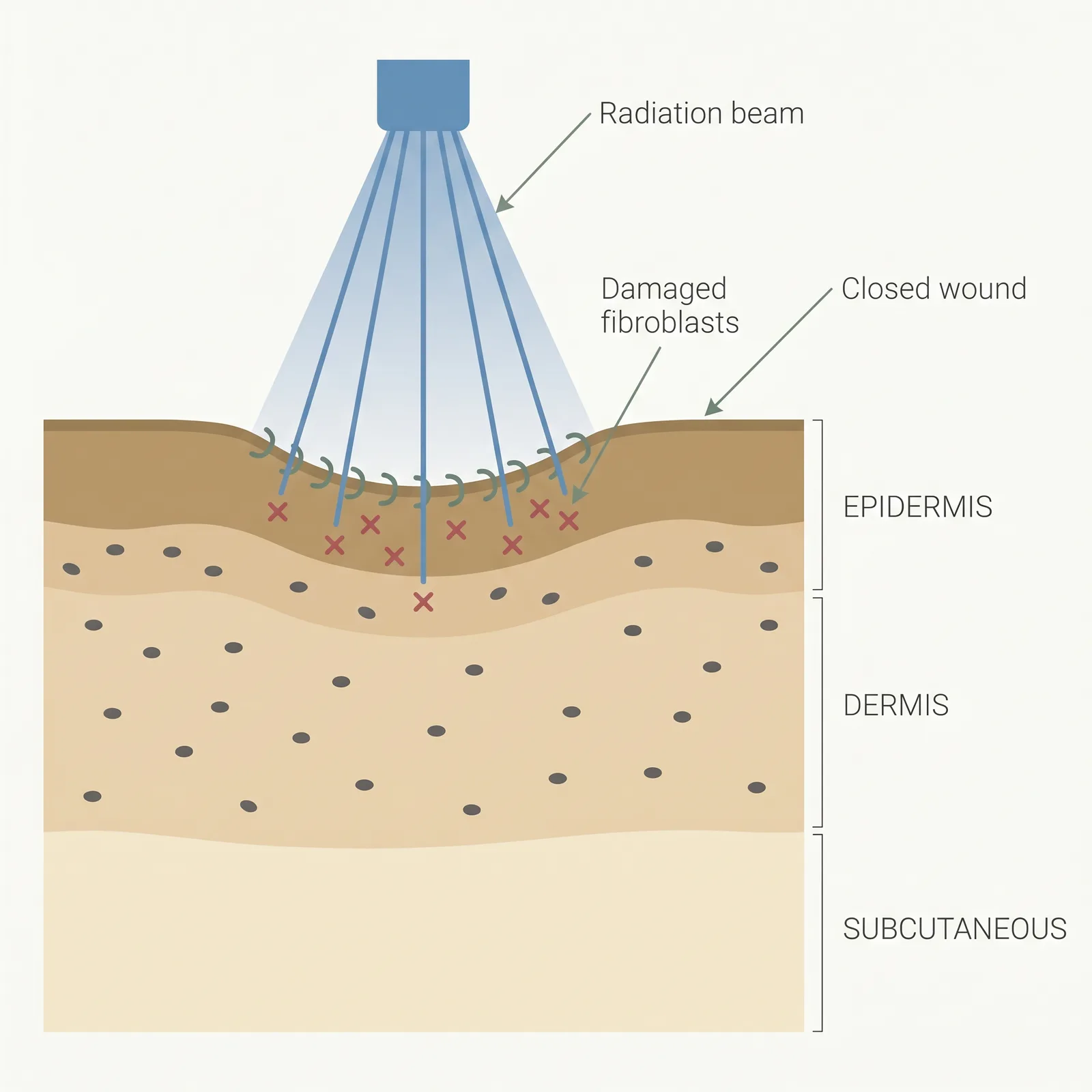
Radiation damages the DNA of rapidly dividing fibroblasts in the fresh surgical wound, interrupting the proliferative phase of wound healing that would otherwise progress into keloid regrowth. The timing is critical: fibroblasts are most radiosensitive in the first 24-72 hours after excision when they are dividing most rapidly, which is why radiation protocols are scheduled immediately post-operatively rather than weeks later. The dose (typically 12-20 Gy total, given in 3-5 fractions) is too low to trigger the chronic skin damage or secondary malignancy risks seen in historical high-dose scar radiation, but high enough to suppress the fibroblast signalling cascade that drives keloid recurrence. Electron beam is preferred for superficial sites because it drops off sharply with depth, sparing deeper tissues. Brachytherapy uses a catheter placed directly in the wound bed to deliver a precise, localized dose — useful on curved or deep sites where external beam has line-of-sight limits. Radiation is almost always an adjunct to surgery, not a standalone treatment for an existing keloid.
- 1Timed delivery. 12–20 Gy is delivered in 3–5 fractions, starting within 24–72 hours of surgical excision.
- 2Targets proliferating cells. Radiation preferentially damages rapidly dividing fibroblasts in the fresh wound bed.
- 3Interrupts regrowth. The signaling cascade that would normally rebuild the keloid is dampened, lowering recurrence.
Typical protocol
Common external-beam regimens deliver 12-20 Gy in 3-5 daily fractions, starting within 24-72 hours of excision. High-dose-rate brachytherapy regimens deliver similar total dose in 1-3 shorter sessions via a catheter in the surgical wound. Site-specific dosing: higher for high-tension areas (chest, shoulder, suprapubic) and lower for ear, scalp, and extremities.
- Time to results
- Wound healing over 4-8 weeks; recurrence risk is assessed at 12-24 months, when the majority of keloids that are going to come back will have done so.
- Accessibility
- limited
- Recurrence
- 10-25% with adjunct radiation after excision, versus 45-100% for excision alone
- Insurance
- sometimes
Best for
- • Recurrent keloids that have failed two or more prior treatment courses
- • Large keloids where excision is the only realistic volume-reduction option
- • High-tension body sites with very high recurrence risk (chest, shoulder, sternum, suprapubic)
- • Adult patients (generally avoided in pediatric and adolescent cases)
- • Keloids in sites where long-term steroid injection is impractical
- • Patients who understand and accept a small long-term oncology risk in exchange for a big recurrence drop
Limitations to know
Combining with other treatments
Radiation is essentially always paired with excision — it is not used as monotherapy on an existing keloid because the fibroblasts in a mature, stable keloid are not dividing fast enough to be reliably suppressed. The excision + radiation combination is one of the most effective recurrence-reduction protocols documented in the keloid literature, but it is also the most resource-intensive and carries the highest barrier to access. Some regimens layer post-op intralesional triamcinolone at 4-6 weeks after radiation as additional insurance against recurrence. Silicone sheeting and pressure therapy are commonly added during the healing phase. Radiation is usually not combined with laser or 5-FU in the same course.
Evidence sources
Postoperative Radiotherapy for Keloids: A Meta-Analysis
2017Mankowski P, Kanevsky J, Tomlinson J, et al. · Annals of Plastic Surgery
Pooled analysis of 33 studies and over 2,500 keloids: adjuvant radiotherapy after excision produced an overall recurrence rate around 20% versus over 70% for excision alone — one of the largest effect sizes in the keloid literature.
View source →Keloid Treatment by Surgical Excision and Immediate Postoperative Single-Fraction Radiotherapy
2009Ogawa R, Yoshitatsu S, Yoshida K, Miyashita T · Plastic and Reconstructive Surgery
Site-specific dosing of post-op electron beam radiation (15-20 Gy depending on anatomical site) produced recurrence rates of 10-25% across a large keloid cohort — the foundational paper behind modern site-based dosing protocols.
View source →High-Dose-Rate Brachytherapy in the Treatment of Keloids
2007van de Kar AL, Kreulen M, van Zuijlen PP, Oldenburger F · Plastic and Reconstructive Surgery
HDR brachytherapy immediately post-excision produced recurrence rates around 15% in recurrent keloids, with excellent cosmetic outcome — establishing brachytherapy as a viable alternative to external beam for select sites.
View source →Radiation Therapy for Keloids: An Updated Review
2013Shen J, Lian X, Sun Y, et al. · Radiation Oncology
Systematic review confirming that biologically effective dose (BED) is the key variable driving recurrence outcomes; BED ≥30 Gy reliably produces recurrence rates under 20% with acceptable safety profile at doses used for keloid work.
View source →
Frequently asked questions
Is radiation therapy for keloids safe? What about cancer risk?
At keloid doses (12-20 Gy total, delivered superficially), the secondary malignancy risk is small but not zero. Published cohort studies tracking patients for 10-20 years report a handful of radiation-related tumours in a few thousand treated keloids — meaningfully above zero, well below most other adult radiation indications. The consensus is that the risk is acceptable for adults when weighed against a recurrence drop from 70-100% to 10-25%, but it is why radiation is not offered for children, for keloids overlying the breast or thyroid without shielding, or for cosmetic-only cases where less aggressive options are viable. Discuss your specific site with the radiation oncologist before deciding.
Why does the timing after surgery matter so much?
Fibroblasts in a fresh surgical wound divide rapidly during the first 24-72 hours as the healing cascade ramps up, and dividing cells are far more sensitive to radiation than resting cells. That window is when a single or short course of low-dose radiation can meaningfully interrupt the signalling that drives keloid regrowth. Wait a week and the same dose no longer does much. This is why protocols demand radiation start within 24-72 hours post-excision, and why it's critical to coordinate surgical and radiation schedules before you commit to either.
External beam vs brachytherapy — how do they compare?
Superficial electron beam is the more common, cheaper option and works well for flat, accessible sites like the chest, shoulder, and extremities; it is delivered externally so there are no catheters or additional wound trauma. High-dose-rate brachytherapy uses a thin catheter placed into the wound bed immediately at closure, and delivers radiation from the inside out — this gives a more precise dose distribution for curved or deep sites (earlobes, posterior neck, ear cartilage) but requires a brachytherapy suite and specialized team. Recurrence rates are similar between the two when the dose is properly calibrated; the choice is mostly anatomical and institutional.
What does the treatment actually feel like?
The radiation itself is painless — you lie still for a few minutes while a machine delivers the dose, similar to an X-ray. You'll feel nothing during the beam. The discomfort in the first 1-2 weeks is mostly from the surgical wound, not the radiation. Expect the treated skin to become pink or darker, dry, and slightly itchy over the course of the sessions and for a few weeks afterward. Long-term changes include mild persistent hyperpigmentation and occasional small telangiectasias (broken capillaries) at the site.
Will insurance cover it?
Sometimes. Coverage is most likely when the keloid is recurrent, symptomatic, or functionally impairing and the radiation is documented as medically necessary adjuvant therapy rather than cosmetic. Ask the surgical and radiation offices to pre-authorize before scheduling surgery — cost ranges from roughly $1,500 for a simple electron-beam course at an academic centre to $8,000+ for brachytherapy at a specialty clinic. If cost is the barrier, alternatives worth discussing with your dermatologist include post-excision triamcinolone + 5-FU protocols, which have a lower recurrence-reduction effect but are more accessible.
Medical disclaimer
ScarInsight provides educational information about scar and keloid treatments based on published research. This content is not intended to diagnose, treat, or prevent any medical condition. Individual results vary. Treatment decisions should be made in consultation with a qualified dermatologist or healthcare provider who can evaluate your specific situation. ScarInsight is not a healthcare provider and does not offer medical advice.