Cryotherapy (Liquid Nitrogen)
Last reviewed: April 2026
Evidence rating reflects the quality and volume of research — not how well the treatment works. How I grade evidence →
Controlled freezing of keloid tissue with liquid nitrogen, delivered either by contact spray to the surface or through an intralesional probe placed inside the scar. Most often used as an adjunct to steroid injections, cryotherapy physically disrupts the dense fibroblast-rich core of a keloid and softens it so subsequent therapies work better.
How it works
Freezing to around -20°C to -40°C triggers three overlapping effects: direct cell death from intracellular ice formation, vascular stasis that starves the scar of blood supply, and a remodeling response as the tissue thaws and is replaced. Contact (spray) cryotherapy reaches only the upper 1-2 mm of the scar, which is why multiple cycles are needed. Intralesional cryotherapy uses a hollow needle-probe inserted into the keloid core, freezing the scar from the inside out — this reaches deeper tissue more uniformly, spares the overlying epidermis, and reduces the hypopigmentation risk that limits contact cryo in darker skin tones. Both techniques also mechanically loosen the collagen network, which is why cryo is often used immediately before a steroid injection — the softened, oedematous tissue allows the corticosteroid to disperse more evenly throughout the scar rather than pooling at the injection point.
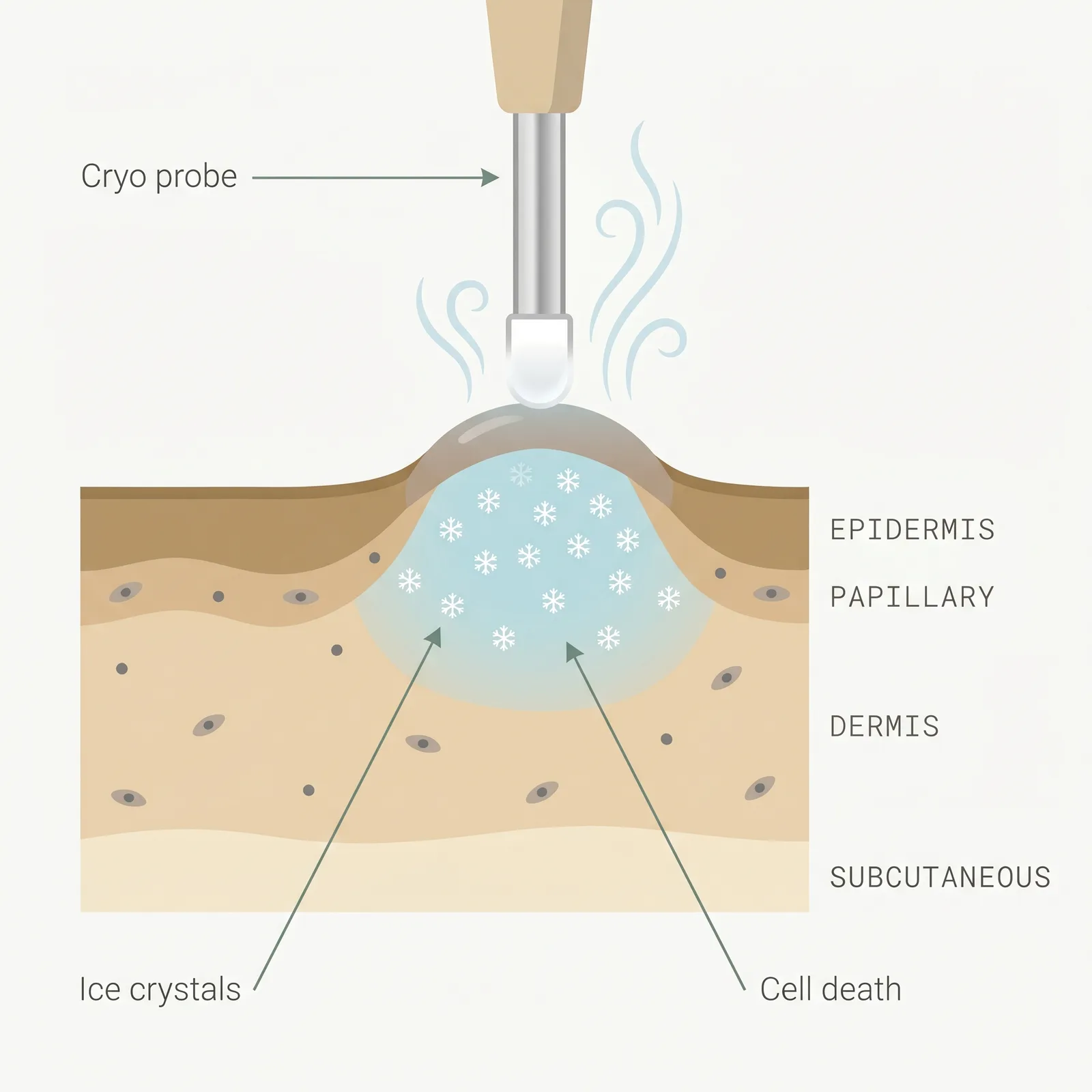
- 1Controlled freeze. Liquid nitrogen applied by contact spray or intralesional probe drops scar tissue below −20°C.
- 2Ice crystal injury. Freezing causes cell death and vascular stasis inside the fibroblast-rich core of the keloid.
- 3Remodeling. Repeat cycles over months flatten the scar; intralesional probes reach deeper tissue than surface spray.
Typical protocol
Contact cryotherapy: 10-30 second freeze cycles, 2-3 cycles per visit, repeated every 3-4 weeks for 3-10 sessions. Intralesional cryotherapy: a single probe session lasting 15-25 minutes, sometimes repeated once at 6-12 months. Cryo-assisted steroid injection: a short freeze cycle immediately before triamcinolone injection to soften the tissue.
- Time to results
- Visible flattening over 2-6 months; most studies report primary endpoints at 6 months.
- Accessibility
- specialist required
- Recurrence
- 20-40% with contact; lower with intralesional (often reported around 15-25%)
- Insurance
- sometimes
Best for
- • Small to medium keloids under 2 cm
- • Keloids that have not responded to steroid injections alone
- • Dense, fibrotic scars where cryo-assisted steroid dispersion is useful
- • Patients with lighter skin tones where pigmentation change is a smaller concern
- • Earlobe and extremity keloids where the probe can be placed cleanly
- • Adjunct to steroid injections (cryo softens tissue for better drug distribution)
Limitations to know
Combining with other treatments
The strongest evidence for cryotherapy is in combination with intralesional steroid. A short contact freeze immediately before triamcinolone injection (the 'cryo-assisted' technique) softens dense keloid tissue so the steroid disperses evenly rather than pooling, which improves flattening and can allow a lower steroid dose with fewer atrophy side effects. Intralesional cryotherapy is sometimes used as a single-session alternative when repeated steroid injections have stalled. Cryo is also used after debulking surgery on small keloids, and pairs with silicone sheeting during the healing phase.
Evidence sources
Intralesional Cryotherapy for Keloid and Hypertrophic Scars: A Systematic Review
2015van Leeuwen MCE, Bulstra AEJ, Ket JCF, et al. · Plastic and Reconstructive Surgery - Global Open
Intralesional cryotherapy achieved substantial volume reduction (around 50-60% on average) in most keloids with lower recurrence than surface cryo and a lower rate of permanent hypopigmentation.
View source →Comparison of Cryotherapy Plus Intralesional Steroid vs Steroid Alone for Keloids
2001Yosipovitch G, Widijanti Sugeng M, Goon A, et al. · Journal of the European Academy of Dermatology and Venereology
Combination cryotherapy plus triamcinolone produced greater scar volume reduction than steroid injection alone, with most patients showing more than 50% flattening at 6 months.
View source →Intralesional Cryosurgery for Treatment of Keloid Scars: A Prospective Study
2003Har-Shai Y, Amar M, Sabo E · Plastic and Reconstructive Surgery
A single intralesional cryotherapy session produced an average 51% scar volume reduction at 18 months, with intact pigmentation in most patients — the seminal trial behind modern intralesional devices.
View source →Cryotherapy in the Treatment of Keloids and Hypertrophic Scars
1993Zouboulis CC, Blume U, Büttner P, Orfanos CE · Archives of Dermatology
Long-term follow-up of contact cryotherapy showed flattening in 50-70% of keloids but a notable rate of persistent hypopigmentation, establishing the risk profile that drove the move toward intralesional techniques.
View source →
Frequently asked questions
Contact cryotherapy vs intralesional cryotherapy — which is better?
Intralesional is the better option when it is available. It reaches the full depth of the keloid in a single treatment, preserves the overlying skin and its pigment, and typically needs only one or two sessions versus the 3-10 visits contact cryo often requires. Contact cryo is more widely available and cheaper per session but is largely limited to small, surface-level keloids and carries a meaningful hypopigmentation risk. If you have darker skin or a thick keloid, seek out a clinic that offers intralesional cryo.
How painful is cryotherapy?
Most patients rate the freeze itself at 3-4 out of 5 — a sharp, deep cold that intensifies as the tissue freezes and often peaks during the thaw. Intralesional cryotherapy is usually done under local anaesthesia because the probe is in the scar for 15-25 minutes. Contact spray is shorter but can still sting for a few minutes afterward. Expect soreness and a throbbing sensation for 24-48 hours, and weeping, crusting, or blistering at the site for up to 2 weeks.
Will cryotherapy cause permanent skin discolouration?
It can. Contact cryotherapy damages melanocytes in the epidermis, which is why hypopigmentation — lighter patches of skin — is the most common lasting side effect, especially in Fitzpatrick IV-VI skin tones. In some people this fades over 12-24 months; in others it is permanent. Intralesional cryotherapy has a much lower pigmentation risk because the freeze is delivered from inside the scar and largely spares the epidermis. If you are concerned about pigmentation, ask specifically which technique your dermatologist uses.
How does cryo-assisted steroid injection work?
Dense keloid tissue resists injection — the steroid tends to pool or leak back out. A brief freeze cycle (usually 10-15 seconds of contact spray) immediately before the injection makes the scar temporarily softer and more porous, so triamcinolone disperses more evenly through the tissue. In practice this often means better flattening per session, less need for high steroid concentrations, and fewer steroid side effects like atrophy or telangiectasia. It is one of the most common uses of cryo in keloid clinics today.
How do I know if cryotherapy is working?
Expect the scar to look worse before it looks better. The immediate effect is swelling, crusting, and blistering for 1-3 weeks. Real flattening begins around 6-12 weeks as the damaged tissue remodels, and final outcome is usually judged at 6 months. Signs cryo is working include a gradual reduction in height, softer feel, and fading of the redness. If there is no perceptible change after two full contact sessions or three months post-intralesional, escalate to a combination protocol rather than continuing monotherapy.
Medical disclaimer
ScarInsight provides educational information about scar and keloid treatments based on published research. This content is not intended to diagnose, treat, or prevent any medical condition. Individual results vary. Treatment decisions should be made in consultation with a qualified dermatologist or healthcare provider who can evaluate your specific situation. ScarInsight is not a healthcare provider and does not offer medical advice.